
The use of CBCT at the diagnostic and treatment planning stage allows to detect presence of refractory endodontic pathology root by root in multicoated teeth. Teeth affected by pathology in one root only due to the presence of missed anatomy cannot be re-treated surgically and a selective orthograde re-rct approach can be opted for.
The use of the Bull-Y Re-Treaty file from Perfect Endo allows “dry” desobturation without using solvents, this approach is very efficient and ideal in cases where the obturation present in the healthy roots should not be disrupted. Dentine structure economy is also recommended, this approach significantly differs from the nonsensical restricted and ninja approaches: access cavity needs to be convenient but as wide as practical to achieve apical disinfection.
Refractory endodontic infection are mostly caused by residual endodontic infection. Among the several reasons for endodontic failure missed anatomy is a major culprit (Nair 2006). An eighty-two year old male with clear medical history, was referred by his general practitioner for persisting fistulous tract in the lower right quadrant. Fistulography long cone periapical revealed unclear origin and a large periapical lesion encompassing both the 45 and 46. The primary RCT on the 46 was carried out in 2011 by an Endodontic specialist, a year later due to non resolving lesion the 45 was treated as well. Prior to committing to any form of further treatment a small FOV CBCT was prescribed. In particular detection of erratic anatomy as the presence of a middle medial canal is very important. The middle medial canal is present in 13.3% of mandibular molars (Honap et al 2020). Alternative approaches may include the use of print and try technique that may aid even further in localising the missing anatomy (Tonini et al 2021). A non treated mesio-buccal canal in the mesial root of the 46 was visualised on the CBCT scan, whereas a merging middle mesial canal was filled as main canal together with the mesio-lingual. Presence of a completely empty canal system discouraged the surgical re-treatement approach (that could efficiently address also the lesion encompassing the 45). A staged approach with non-surgical re-RCT of the 46, potentially followed by re-rct of the 45 was opted for. The use of the Perfect Re-Treaty sequence as demonstrated in a previous article (http://endodontics.styleitaliano.org/conservative-retreatment-using-re-treaty/) allows a conservative re-treatment approach that, thanks to the Bull-Y file efficiently removes the pre-existing obturation material without the need to use solvents and minimising the radicular dentine removal. Subsequently The Skinn-Y can be utilised to regain apical patency, followed by the shaper 1 and 2 (and optionally the Shaper3) to complete the shaping and removal of the apical infected dentine, at limited expense of the coronal dentine thanks to the 5% taper. A fast and efficient shaping phase allows to indulge longer in the chemodebridement phase. A final obturation with bio ceramic single cone technique was carried-out.
 Fig. 1
Fig. 1
File sequence for the Re Treaty System, to be noted the shorter desobturator file the Bull-Y and the pantency/scouting Skinn-Y file allowing gentle and still resilient rotary scouting. The shaper can negotiate complex anatomy with maximum dentine preservation without compromising the necessity to remove infected dentine.
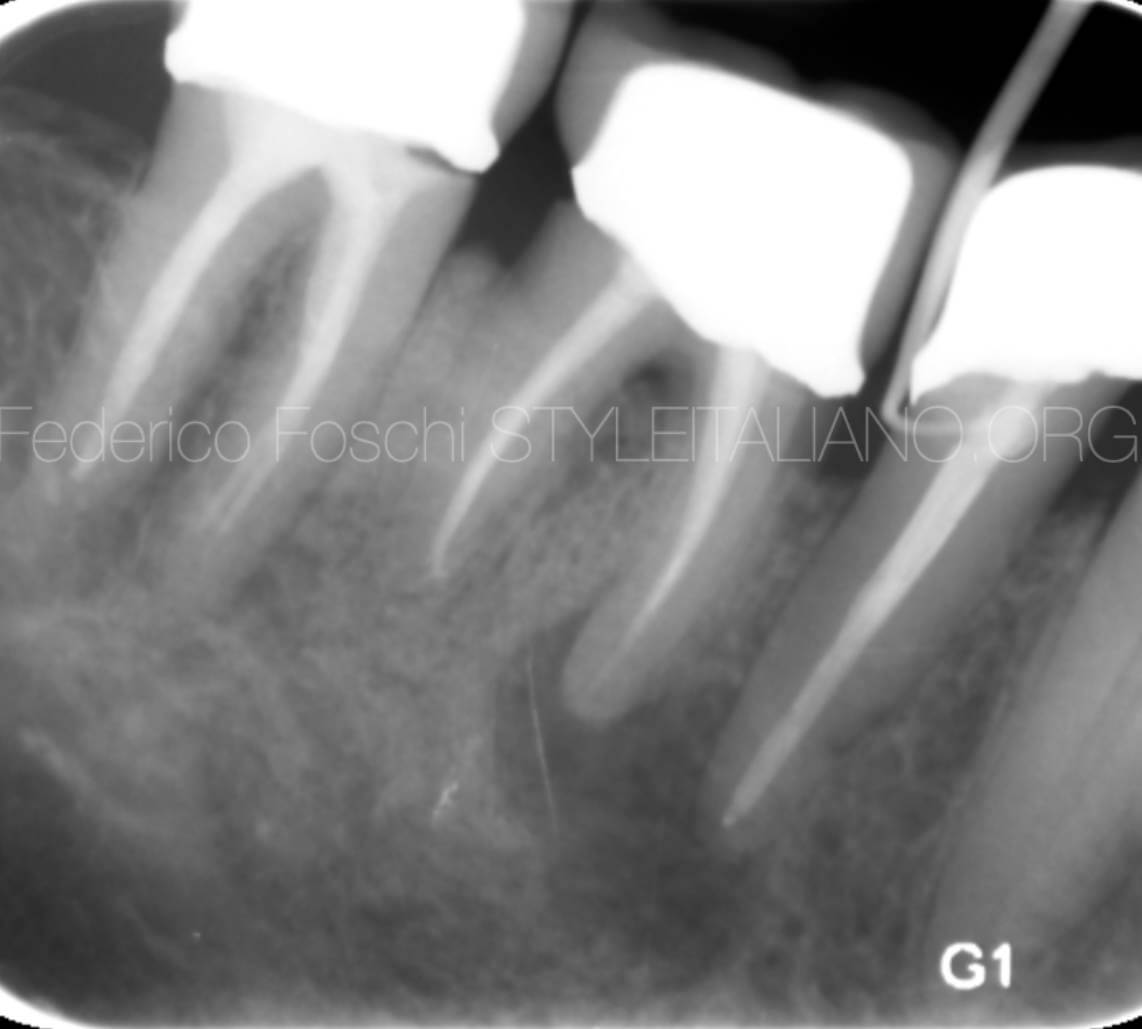 Fig. 2
Fig. 2
Pre-operative long cone periapical x-ray revealing a large lesion encompassing the 45 and 46 with coronal fistulous tract
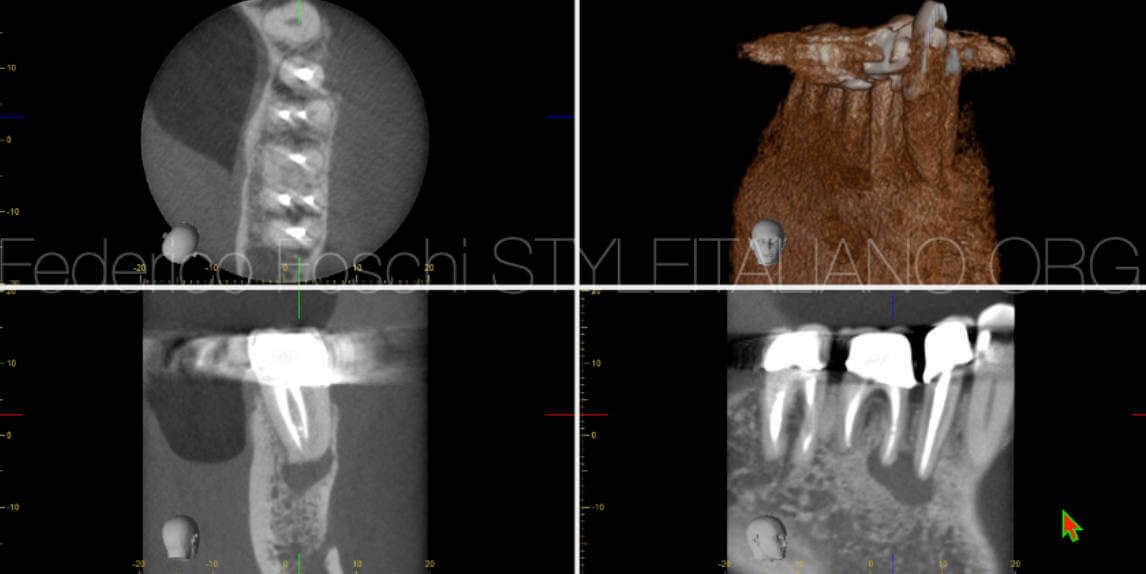 Fig. 3
Fig. 3Small FOV CBCT taken with XJ800 Morita revealed a missed MB canal in the medial root, in particular the MM canal was filled instead of the actual MB. No lesion was present at the distal root of the 46, which contained a well condensed root canal filling.
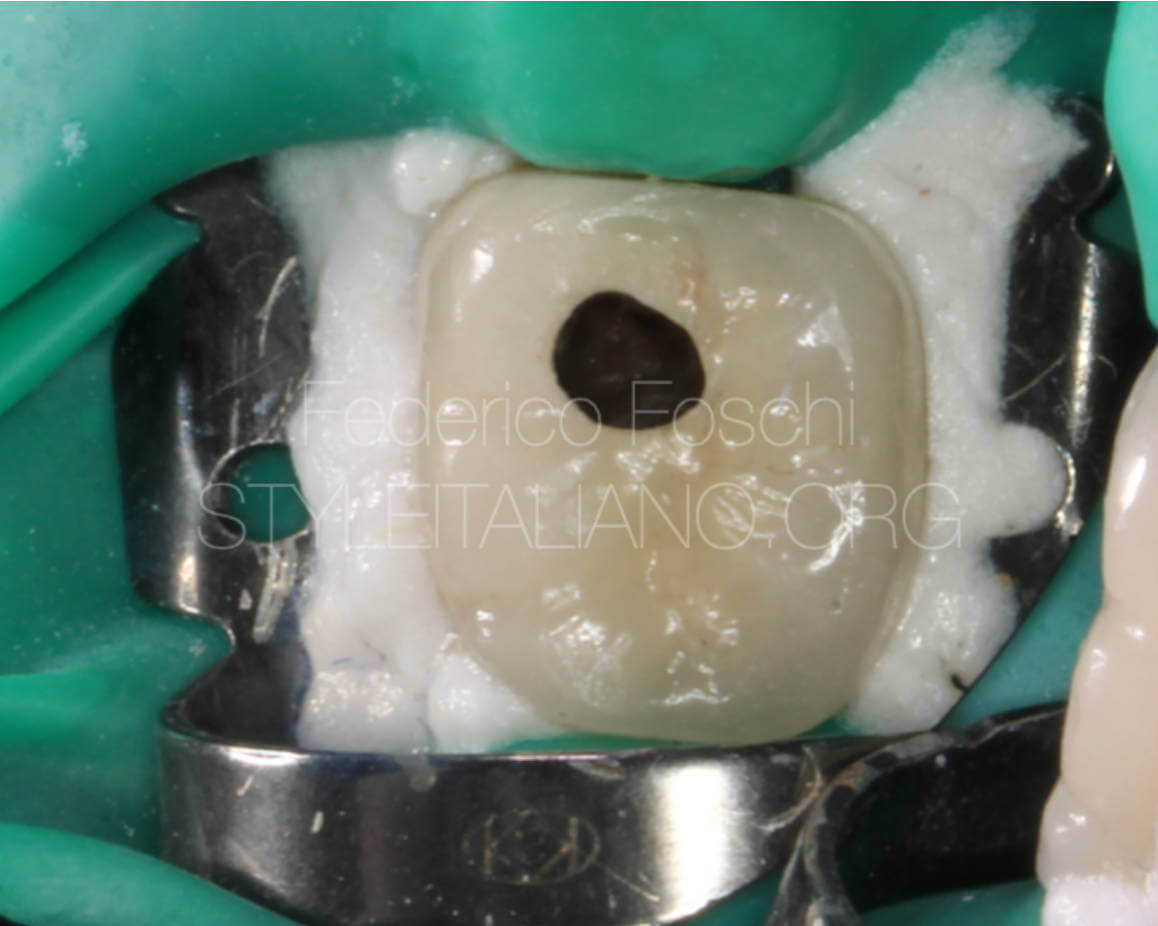 Fig. 4
Fig. 4
A mesialised non restricted access cavity was opted for as the distal root was not affected by endodontic pathology
Intraoperative clincial stages of the shaping up to the irrigant activation
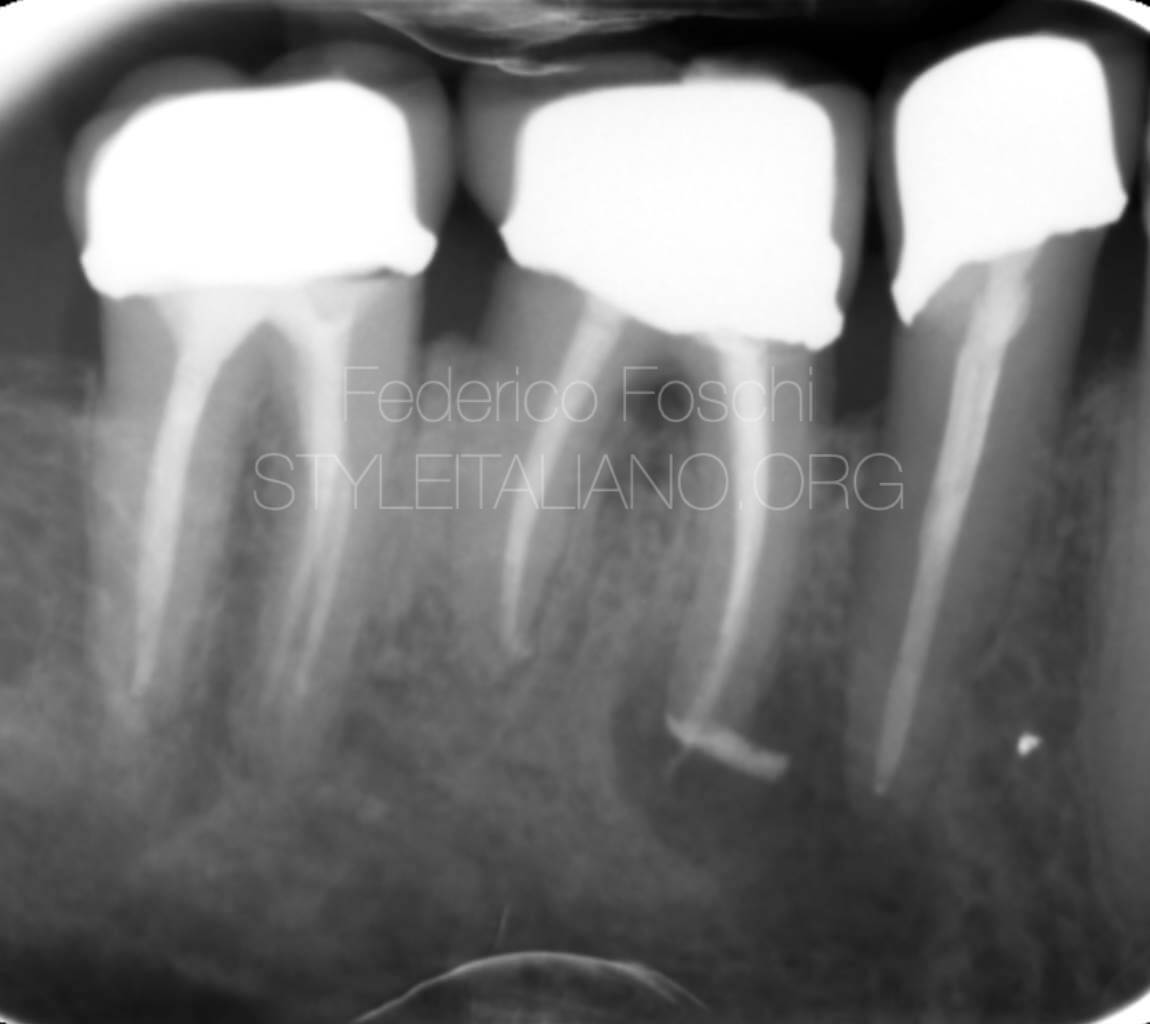 Fig. 5
Fig. 5
Final obturation with bio ceramic sealer surplus
 Fig. 6
Fig. 6
Parallax view of the root canal system in the mesial root of the 46 following the selective re-treatment.
A selective re-treatement approach can be opted in case of missed anatomy isolated to one single root in the absence of pathology on the other one. A novel re-treatment martensitic NiTi system called Re Treaty, introduced by Perfect allows to efficiently desobturate and remove the pre-existing obturation material and regain apical patency prior to the final shaping and debridement of the canals.
Nair PN. On the causes of persistent apical periodontitis: a review. Int Endod J. 2006 Apr;39(4):249-81. doi: 10.1111/j.1365-2591.2006.01099.x. PMID: 16584489. Honap MN, Devadiga D, Hegde MN. To assess the occurrence of middle mesial canal using cone-beam computed tomography and dental operating microscope: An in vitro study. J Conserv Dent. 2020 Jan-Feb;23(1):51-56. doi: 10.4103/JCD.JCD_462_19. Epub 2020 Oct 10. PMID: 33223642; PMCID: PMC7657433. Tonini, Riccardo & Xhajanka, Edit & Giovarruscio, Massimo & Foschi, Federico & Boschi, Giulia & Atav Ates, Ayfer & Cicconetti, Andrea & Seracchiani, Marco & Gambarini, Gianluca & Testarelli, Luca & Pacifici, Luciano. (2021). Print and Try Technique: 3D-Printing of Teeth with Complex Anatomy a Novel Endodontic Approach. Applied Sciences. 11. 1511. 10.3390/app11041511.







Whether you are a beginner or an expert, this event will give you the opportunity to learn and progress

Product consultant one-on-one service
Free product solutions
Professional team meticulous answer



© 2024 dental-perfect.com. All Rights Reserved.Shenzhen Perfect Medical Instruments Co. Ltd










