

 Correct endodontic treatment has to follow several parameters: proper diagnosis, isolation of operating field, full chemo-mechanical preparation of the complex endodontic system, three-dimensional obturation of the root canals and finally the post endodontic restoration. Respecting all these parameters, short- and long-term success can be achieved. Failure to follow the protocol in any of the above steps can lead to failure of the endodontic treatment.
Correct endodontic treatment has to follow several parameters: proper diagnosis, isolation of operating field, full chemo-mechanical preparation of the complex endodontic system, three-dimensional obturation of the root canals and finally the post endodontic restoration. Respecting all these parameters, short- and long-term success can be achieved. Failure to follow the protocol in any of the above steps can lead to failure of the endodontic treatment.
Reading a preoperative periapical radiograph is of utmost importance. Though, they are 2 dimensional but do give us an idea of what approximate type of root canals we will be dealing with in a particular case. here the article introduction.
A thorough knowledge of root canal morphology and a good anticipation of their possible morphologic variation will help to reduce endodontic failure.
Description of the case
The case has been referred for completion of the initiated root canal therapy as the patient was not getting the relief from pain even after access cavity initiation 3 weeks before.
Patient information
Age:26-year old
Gender: Female
Medical history: non-contributory
Identification: Left maxillary First molar (Tooth 26)
Dental history : Chief complaint: I was having pain while eating. Though root canal was started outside but no relieve in pain is there and I am still in pain.
Clinical examination findings:
The tooth 26 is tender to percussion and an initiated access cavity can be seen on the preoperative radiograph. Temporary filling material present occlusally. Periodontal probing was within normal limits.

Fig. 1
The periapical radiograph revealed initiated root canal treatment in 26. Radiopaque material can be seen in the root canals. Palatal root suspected to be untouched. Periapical radiolucency associated with mesiobuccal root. Previously root canal treated 25 short obturation and full coverage post endodontic restoration.

Fig. 2
Superior alveolar nerve block was administered and Buccal infiltration anesthesia was administered, the tooth was isolated with rubber dam isolation and the tooth was seen under the microscope preoperatively
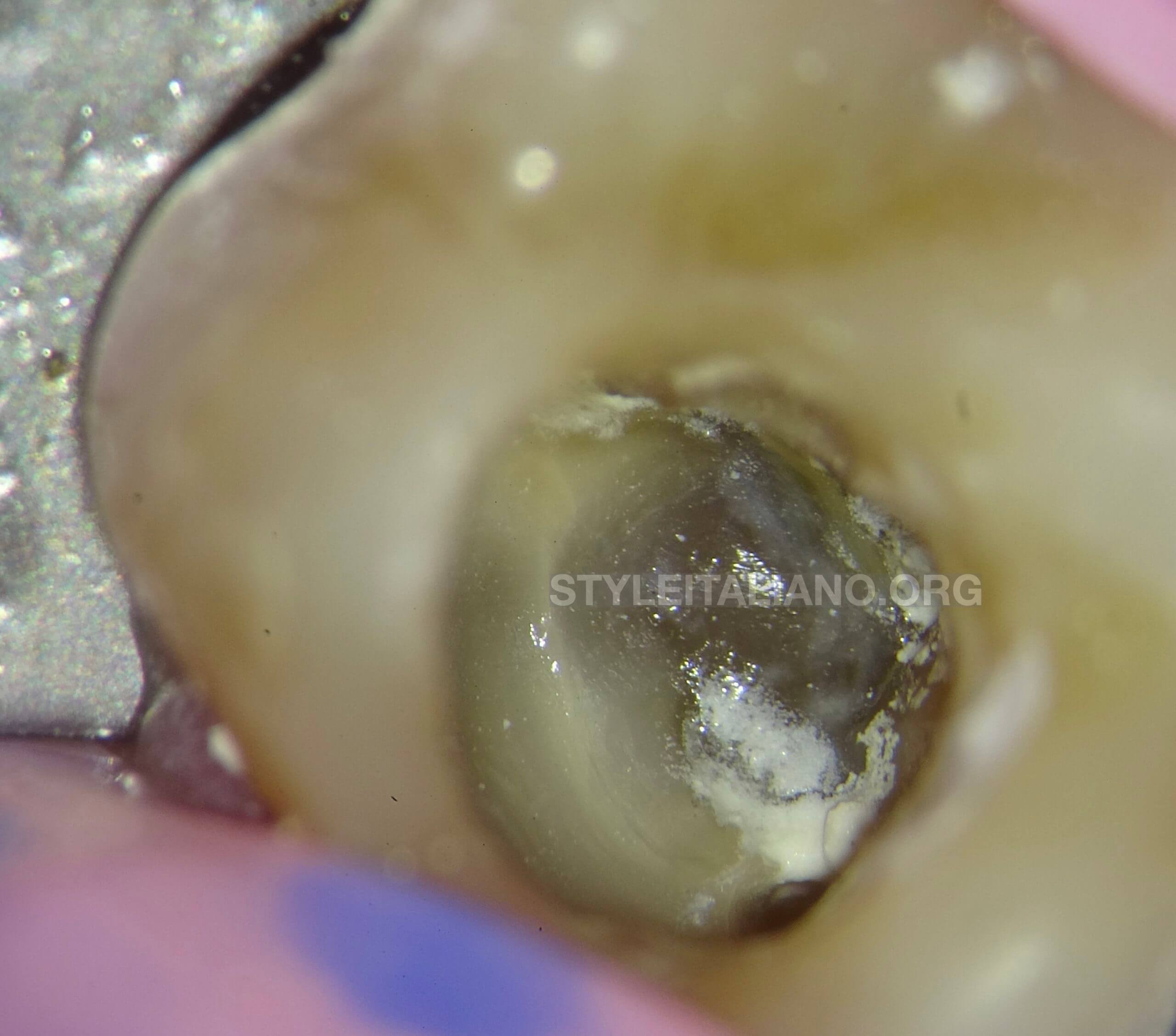
Fig. 3
The first look of the access cavity after removing the temporary restoration.
The access cavity needs to be modified to have straight line access in the Db and Palatal canal respectively.
Modification of the Access cavity done with the help of Endodontic Ultrasonics in order to achieve a straight line access in the Distobuccal and Palatal canal.
Traditionally, most endodontic canal detection procedures have relied on the dentist's tactile dexterity, and mental image of the canal system because the ability to visualize the canal orifices is severely restricted.
Procedure for Locating the Fourth canal:
It is better to use ultrasonic tips designed exclusively for this purpose and not use Access cavity burs..
The ultrasonic tips allow to achieve a better view, furthermore are more conservative than the High speed access cavity burs.
The tip that has to be used for the fourth canal finding has to be small, with diamond or micro machined surface, not-pointed to avoid scratches and perforations of the chamber floor and used with a cooling system to chill the tip and to remove debris.
After the identification of the main canals, the magnification has to be increased (8×) and proceed as follows:
The ultrasonic tip, used with a specific ultrasonic source and set on an average power, will be placed at the area suspected to have an extra canal (in this case MB area), activated and directed towards the palatal canal.
During this phase the tip must be located mesially, where the thickness of dentin is greater to avoid perforations.
The groove depth will be about 0.5–1 mm, while the extension in palatal direction will be about 1–2 mm
Establishing a Glide path is of utmost importance.
10k hand files or the glide path files in the kits of various rotary instruments are the best files.
The files should always be used with lubricant and in a wet canal.
Cleaning and shaping should be carried with rotary files used in sequential manner. Jumping the files can result in creating stress on the instrument being used leading to instrument separation or various other endodontic mishaps.
Introducing a well lubricated G2 file in a sequential manner helps to clean and shaped and achieve a uniformly tapered canals unto the working length.
Never ever force the files inside the canal. Let them glide their path inside the canal predetermined by Glide path files.
Choosing a larger file for large canals is done in order to perform adequate dentin removal followed by adequate Irrigation to clear off the debris and disinfect the root canal system 3 dimensionally.
Once the canals are cleaned and shaped, master cone fit should be verified on the radiograph.
If using a Bioceramic sealer then the canals can be left a bit moist and sealer can be injected inside the canals. Master cone introduced passively and cut with the heated plugger.
Gentle vertical condensation of the cut Gp helps for better adaptation of the GP to the dentine walls.
Finally the pulp chamber should be cleaned and excess sealer or Gutta percha should be removed from the pulp chamber.

Fig. 4
The Pulp chamber should be rinsed thoroughly and cleaned of any excess sealer or Gutta percha.
The GP should end coronally at the orifice
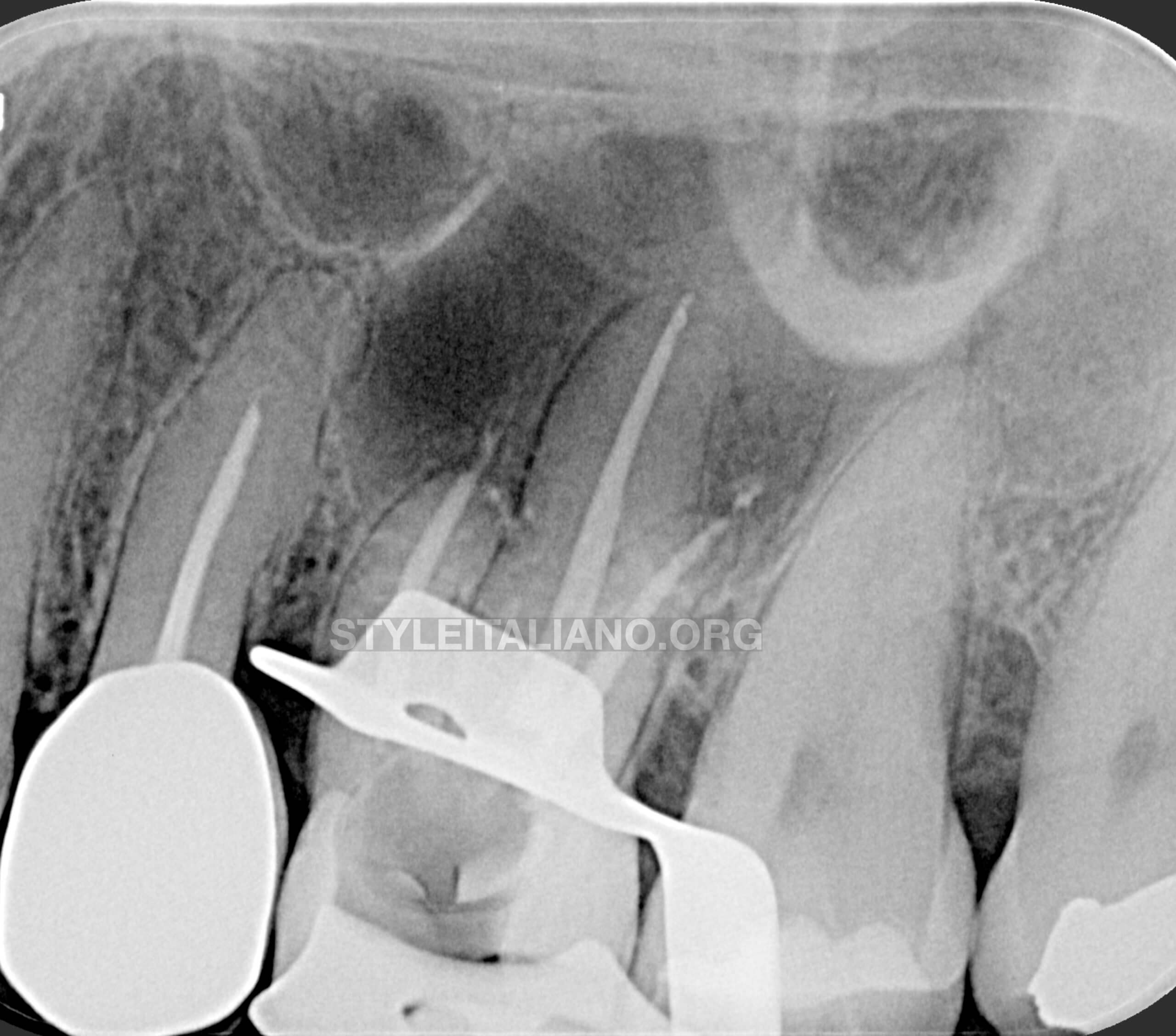
Fig. 5
Radiographic Verification of the obturation.
Conclusions
The success of Endodontic therapy depends upon adequate shaping, proper 3D cleansing followed by a correct obturation of the complex system of root canals with preferred obturation technique.
The manual and mechanical files do not come in complete contact with the dentine walls therefore more time to the cleansing and disinfection phase after the shaping step should be given.
Through the modern techniques of disinfection the three-dimensional cleansing of all the inaccessible endodontic areas can be achieved.
Even if a complete bacteria removal is not achieved, it will be too low to allow the defense system action to proceed to healing and then get the success in short and long term.
Following a proper Endodontic protocol, using rotary instruments in their preferred sequential manner and using adequate irrigation along with magnification helps the dentist to achieve good results in root canal treatment.
Bibliography
Ghoddusi J, Mesgarani A, Gharagozloo S. Endodontic re-treatment of maxillary second molar with two separate palatal roots: a case report. Iranian endodontic journal. 2008;3(3):83.
Witherspoon DE, Small JC, Regan JD. Missed canal systems are the most likely basis for endodontic retreatment of molars. Tex Dent J. 2013 Feb 1;130(2):127-39.
Eskandarinezhad M, Ghasemi N. Nonsurgical endodontic retreatment of maxillary second molar with two palatal root canals: a case report. Journal of dental research, dental clinics, dental prospects. 2012;6(2):75.
Wolcott J, Ishley D, Kennedy W, Johnson S, Minnich S. Clinical investigation of second mesiobuccal canals in endodontically treated and retreated maxillary molars. Journal of endodontics. 2002 Jun 1;28(6):477-9.







Whether you are a beginner or an expert, this event will give you the opportunity to learn and progress

Product consultant one-on-one service
Free product solutions
Professional team meticulous answer



© 2024 dental-perfect.com. All Rights Reserved.Shenzhen Perfect Medical Instruments Co. Ltd









